
Case Study
Lighting Solutions for Healthcare
How our Sanitising Lighting Solutions reduce the bacterial load inside of the First Aid building of Rome's Leonardo Da Vinci airport.
Our lights continuously sanitise without sterilising, therefore reducing the risk of infection whilst making them completely safe for humans and animals. They are effective against bacteria and viruses in the air and on surfaces, making the areas they are used in considerably healthier. The following case study explores the effect of the lights on a real-life First Aid building in Rome airport.
The Environment
In recent years, airports have assumed an increasingly important role in containing biological risks. The increase in the flow of goods and people from and to every part of the world has exacerbated the risk of spreading biological agents from different areas of the world. The issue includes both sick travellers, who have not yet shown the symptoms of any infection and healthy carriers of some biological agents (which are not distinguishable from other travellers), to clinically healthy travellers who naturally carry some symbiotic biological agents that are safe for them but potentially harmful for other populations. Not to mention the risk inherent in the handling by the operators inside the airport of goods and the promiscuity during the baggage collection phase.
Unfortunately, airports are also facing risks that are not only linked to their production cycle but also to the risks that potentially derive from aircraft internal systems, such as water tanks or air conditioning systems that are linked to potentially infected waste. The issue of health and safety at work, in health facilities, is a matter of considerable importance and of great complexity from the point of view of its realisation.
Healthcare professionals during their patient care activities are exposed to various risk factors, including in particular, biological. Working in the First Aid ward as a nurse, doctor, auxiliary and managing numerous cases of emergencies during the work shift, involves a considerable commitment both physically and mentally. In such situations, ensuring adequate assistance and at the same time guaranteeing one’s own safety and health at work is not an easy task.
The Emergency Department is an operative unit dedicated to emergency cases in which patients are given first care. This is a bio-risk department in which direct assistance services are performed to patients in conditions of great stress and professional commitment, involving the performance of often invasive activities and the continuous exposure of health workers to biological agents through direct or indirect contact with the patient source. The biological risk in this structure is not given by the deliberate use of microorganisms but by a presence, more or less high, consequent to the work activities and to the numerous presences of subjects who go there to receive assistance.
Background
Here you will find details on the various parts of the First Aid building relevant to the case study. Just open up the box to find out more.
The main entrance is accessed from the external space through an automated sliding glass door. It is the first area you come across when accessing the Hospital, where patients are registered by the staff. The patients, the ambulance crew that responded to the emergency call, and any companion must stop here. Only patients and crew come inside.
In this room the operators register the patients before letting them go into the first aid station, in which they are brought by the ambulance crew. A glass window separates this room from the main entrance.
In this room, the patients have access to the first clinical evaluation, and it can also be used for any minor surgical emergency. Inside the room, there is the examination bed used for all medical assessments when the patient is awake and cooperative and the doctor’s desk.
In this room are hosted patients who, after having been stabilised, require staying under observation for a short period of time (48 hours maximum). The presence of a companion is allowed.
This room communicates directly with the first-aid station (L3) through a door. It hosts the devices for monitoring the most common vital functions (e.g. sphygmomanometer, ECG, etc.) and the PC is used by the medical and nursing staff to record the clinical activities performed on each patient.
This room is for the exclusive use of the medical staff. Doctors use it both for resting and consuming meals.
Method
First of all, the surfaces subject to sampling in the different areas were identified, preferentially choosing the ones that are more suitable, because they are used more frequently or by a high number of living beings. In the studied places, the humidity, the total number of accesses of living beings and the cleaning routine were monitored. Because surface contamination can be caused by both deposition of suspended bioaerosol and contact with contaminated humans and media, the samples have to be collected with nylon swabs moistened by dipping them in sterile saltwater. A 10x10cm disposable sterile mask was used to make sure that the sampling space was always the same. All samples were carried out by a specialized technician Dott. Vincenza Cafaro (Biologist for Vergata University Rome) in the presence of Engineer Marco Braccini (ADR) and Dott. Rosario Valles CSO Nextsense. The technician responsible for the samples always wore a clean medical gown and sterile gloves.
The areas were swiped 20 times back and forth from left to right and back, 20 times from up to down, 20 times diagonally, 20 times diagonally. The following factors were considered before engaging in environmental surface sampling:
- Location of surfaces to be sampled
- Method of sample collection and appropriate equipment for this task
- Number of replicate samples needed, and which control or comparison samples are required
- Parameters of the sample assay method and whether the sampling will be qualitative, quantitative, or both
- Some anticipation of a corrective action plan.
Microbes from the swabs were diluted to 4 ml of saltwater containing peptone before traditional culturing on Plate Count agar plates (PCA) and Chromocult Coliform agar plates. The pour plate technique was used for the determination of total bacteria on PCA to get a detection limit of 4 CFU (colony forming units)/100 cm2. Coliforms were cultured using a spreading technique on Chromocult agar plates with a detection limit of 40 CFU/100 cm2. Incubation was performed for PCA plates at 30°C for 3 d and for Chromocult plates at 37°C for 2 d after the incubation period colonies were counted from the agar plates.
Results
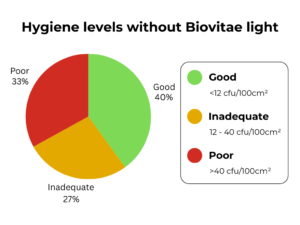
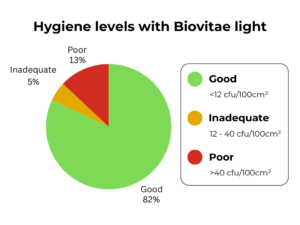
The pie charts below show the total results through the First Aid building.
The bar graph below shows the total results broken down into each room.
")
Findings
In previous hospital studies, we have defined for aerobic heterotrophic bacteria threshold limit <12 CFU/100 cm² for good results at the hospital environmental surface with possible patient contact and 12-40 CFU/100 cm² for inadequate and >40 for poor hygiene (Wirtanen et al. 2012). According to the number of samples in each hygiene category, the use of Our Light has reduced the number of sampling places with poor hygiene from 32.5% to 12.5% and the number of sampling places showing good hygiene has increased from 40% to 82.5% after Our Lights were installed.
So why not talk to us about our solutions for lighting as part of our Healthy Buildings range.
If you’d like to find out more about our approach and experience in creating healthy buildings please do get in touch.